Are you getting the right type of Folate?
With a large percentage of the population not being able to metabolise certain forms of folate, its important to understand what type of folate you need to support your fertility, pregnancy and breastfeeding journey is critical.
The prenatal methyl supplement is designed to support those with the gene variation, providing the correct nutrients and support your system needs.
The prenatal with the highest dose of biologically active folate* (5-MTHF).
Prenatal Methyl Multivitamin is a prenatal, pregnancy and breastfeeding formula specifically formulated with biologically active folate to support a healthy pregnancy, healthy foetal development and placental health.
- levomefolic acid, also know as 5-MTHF is the only biologically active form of folate in the body which does not need to be converted to be used.
- Unisex formula and so suitable for both males and females
5-MTHF does not require enzymatic conversion and can be utilised directly by the body






This prenatal has been designed by Carolyn Ledowsky, Health Scientist, Researcher, Naturopath and Herbalist. Carolyn is dedicated to improving fertility rates around the world and is conducting research on the genetic polymorphisms that might affect the uptake and metabolism of different forms of folate.
Why Choose Prenatal Methyl?
Suitable for

Preconception

Pregnancy

Breastfeeding

Highest Level Of Folate
Our Prenatal Methyl formula is provides the highest level of biologically active folate. This form of folate does not need to be converted by the body to be used.

Does Not Contain Iron
We ensure our product is Unisex, allowing both partners to take the same supplement. As there is no iron in our product, we recommend that you regularly check your iron levels.

Unisex Formula
One supplement for both parents. A simple and easy way to ensure optimal egg and sperm health.

Maintains And Supports A Healthy Pregnancy
The modern diet may lack key nutrients needed in pregnancy. The prenatal Methyl multivitamin can assist in providing the required dietary intake.

Maintains And Supports Healthy Foetal Development
High cell turnover during foetal development places demands on our folate levels. Prenatal Methyl helps ensure you have the levels you need.
Maintains And Supports Placenta Health And Growth
Biologically activated folate may help to ensure a healthy placenta, Prenatal Methyl has the highest level of biologically active folate in the retail market.
Frequently Asked Questions
The Federal Government advises all women thinking of falling pregnant to take a folate based multivitamin for at least a month before pregnancy. It is important to prevent neural tube defects and spina bifida. Both men and women require certain nutrients for optimal egg and sperm health. Folate particularly is required when cell turnover is increased, such as in foetal development.
Sometimes our diet may lack key nutrients and so a multivitamin can assist where dietary intake is inadequate.
Reference: National Health and Medical Research Council (NHMRC)
Prenatal Methyl provides this highest level of biologically active folate (5-MTHF) than any other prenatal available to men and women. 5-MTHF does not need to be converted by the body to be used and therefore we say why not use the most active form of folate available? It is also the form of folate naturally occurring in foods. So in combination with a good nutrient dense diet, Prenatal Methyl may help you meet the increased nutritional demands that occur during pregnancy and breastfeeding.
No Prenatal Methyl does not contain iron as it is a unisex formula and men do no need iron like women.
It is important therefore that you regularly check iron throughout your pregnancy to ensure that your iron is not low. Speak to your Dr about your iron levels on a regular basis.
Yes, Prenatal Methyl is dairy free.
Yes, Prenatal Methyl is gluten free.
Yes, Prenatal Methyl is egg free
Yes, Prenatal Methyl is fish and shellfish free.
Yes, Prenatal methyl is free of genetically modified ingredients.
Both Males and Females should take 3 tablets once per day with water.
Yes, Prenatal methyl is nut free.
Yes, Prenatal Methyl is vegan friendly.
The Vitamin E in this product is soy derived. We do not add extra soy, however there may be traces of soy from the Vitamin E in this product.
Yes, Prenatal Methyl is sulphite free.
Yes, Prenatal Methyl is salicylate free.
Yes, Prenatal Methyl is sugar free.
Yes, Prenatal Methyl is Yeast free.
Activated Folate
This form of folate does not need to be converted by the body to be used
Vitamin D
To support healthy neuromuscular system function
B12
Keep the body’s nerve and blood cells healthy
Choline
Support brain and cognitive development
Betacarotene
Thiamine hydrochloride (Vitamin B1)
Riboflavin sodium phosphate, Equiv Riboflavin (Vitamin B2)
Nicotinamide (B1)
Calcium pantothenate, Equiv. pantothenic acid (Vitamin B5)
Pyridoxal 5- phosphate monodydrate, Equiv.pyridosine (Vitamin B6)
Levomefolate calcium, equiv.levomefolic acid (5-MTHF)
Mecobalamin (Vitamin B12) (co-methylcobalamin)
Hydroxocobalamin (Vitamin B12)
Biotin
Choline bitartrate
Inositol
Ascorbic Acid (Vitamin C)
Colecalciferol Equiv. Vitamin D3
d-alpha-Tocopheryl acid succinate, Equiv.d-alpha-Tocopherol (Vitamin E)
Phytomenadione (Vitamin K1)
Calcium citrate tetrahydrate. Equiv. Calcium
Chromium picolinate, Equiv. Chromium
Magnesium citrate, Equiv. Magnesium
Manganese (II) glycinate, Equiv. Manganese
Sodium molybdate dihydrate, Equiv Molybdenum
Potassium iodide, Equiv Iodine
Selenomethionine, Equiv. Selenium
Zinc citrate dihydrate, Equiv Zinc
Alpha lipoic acid
Ubidecarenone (Coenzyme Q10)
Infertility may be due to a number of factors including, but not limited to, a woman’s advanced age, egg and sperm quality, parental chromosomal anomalies, genetic or metabolic abnormalities of the embryo, or poor uterine receptibility [1].
The potential importance of genetic causes of infertility has resulted in researchers investigating the effect of different genes on sperm and oocyte quality and infertility [2].
The effect of nutrients including folate and food based substances has been extensively researched in relation to fertility and has generated new insights regarding the metabolism of these nutrients, the genes that control them and environmental exposures influencing their bioavailability [3-6].

Why we use methyl folate (5-MTHF) in our prenatal
There are 3 forms of folate on the market
1. Folic acid
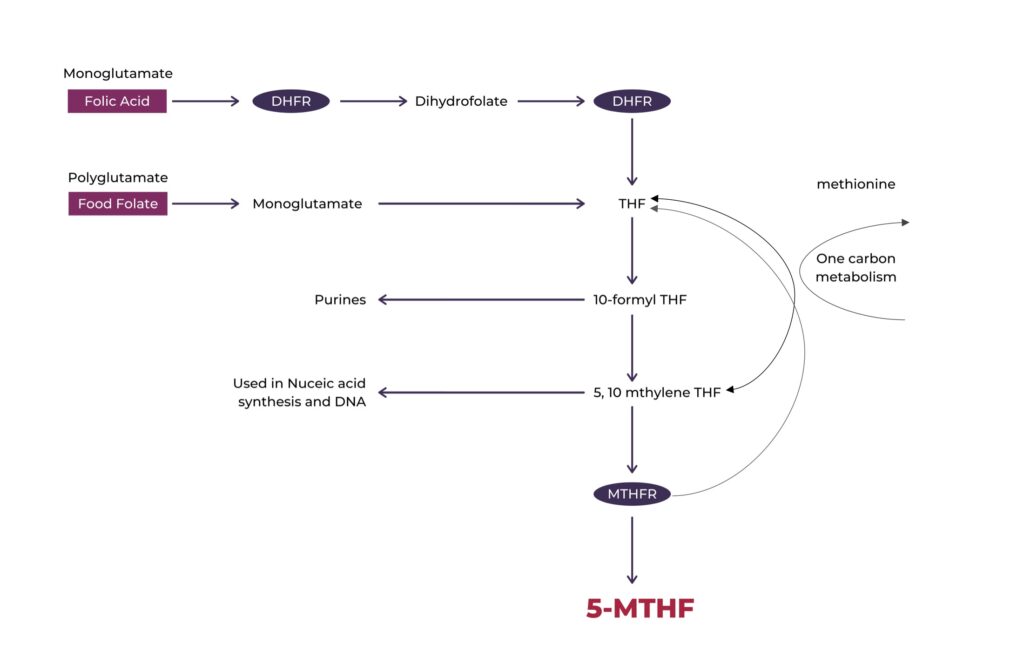
This is the synthetic form of folate. It requires conversion before it can be used in the body [7, 8] and must undergo several metabolic steps (figure 1) to be converted into the active tetrahydrofolate (THF) form and 5-methyltetrahydrofolate (5-MTHF) forms. FA is more stable than natural folates and is cheaper to manufacture which may explain why this form is used in fortification of foods and dietary supplements [9-11]. FA must be first reduced to dihydrofolate (DHF) and then to THF by an enzyme dihydrofolate reducatase (DHFR) [10, 12]. This two-step process to convert FA to THF is slow [13] and easily reaches saturation [14, 15]. This saturation leads to a build-up of FA known as unmetabolized folic acid (UMFA) [16, 17]. UMFA has been found to appear in serum plasma following oral intakes of more than 200mcg of FA. Studies have shown that the amount of FA ingested on a daily basis due to food fortification exceeds original projections [15, 16, 18-21]. The significance of this UMFA is currently unclear, however studies in relation to fertility, pregnancy and breastfeeding suggest it may affect 5-MTHF and folate levels.
Folic acid (FA) has been the traditional form of folate prescribed by Australian practitioners for preconception and pregnancy [4]. Fortification of foods with FA was introduced in Australia to reduce neural tube defects (NTD) and has, by all accounts, been successful [22, 23] . Research, however, has identified that people living in countries with FA fortification of food have an intake that exceeds the original intended dose [9, 15, 24].

2. Folinic acid
This is a metabolically active folate. It doesn’t need the DHFR enzyme, however some people with genetic polymorphisms in some genes in the folate pathway still need to convert it to the biologically active folate 5-MTHF.
3. Methyl folate (methyltetrahydrofolate 5-MTHF)
This is the ONLY biologically active folate in the body. It is naturally found in food like leafy green vegetables [17]. All forms of folate must be converted to 5-MTHF which is the main form of folate found in plasma (around 90%)[12]. MTHF is the biologically active form of folate and is the main form found in the blood, accounting for around 90% [10, 14, 15]. 5-MTHF is critical for methylation required for synthesis of DNA, RNA, neurotransmitter synthesis, proteins and imprinting of genes [9, 25, 26].
Prenatal Methyl is the only Prenatal on the market in Australia with 500mcg of biologically active folate (5-MTHF).
This form of folate can be used directly by the body and does not need to be converted to be utilised by the body.

- Nowak I, Bylinska A, Wilczynska K, Wisniewski A, Malinowski A, Wilczynski JR, et al. The methylenetetrahydrofolate reductase c.c.677 C>T and c.c.1298 A>C polymorphisms in reproductive failures: Experience from an RSA and RIF study on a Polish population. PLoS One. 2017;12(10):e0186022. doi:https://doi.org/10.1371/journal.pone.0186022
- Dobson AT, Davis RM, Rosen MP, Shen S, Rinaudo PF, Chan J, et al. Methylenetetrahydrofolate reductase C677T and A1298C variants do not affect ongoing pregnancy rates following IVF. Human Reproduction. 2007;22(2):450-6. doi:https://doi.org/10.1093/humrep/del396
- Gardiner PM, Nelson L, Shellhaas CS, Dunlop AL, Long R, Andrist S, et al. The clinical content of preconception care: nutrition and dietary supplements. Am J Obstet Gynecol. 2008;199(6 Suppl 2):S345-56. doi:https://doi.org/10.1016/j.ajog.2008.10.049
- Gomes S, Lopes C, Pinto E. Folate and folic acid in the periconceptional period: recommendations from official health organizations in thirty-six countries worldwide and WHO. Public health nutrition. 2016;19(1):176-89. doi:https://doi.org/10.1017/S1368980015000555
- Hanson MA, Bardsley A, De‐Regil LM, Moore SE, Oken E, Poston L, et al. The International Federation of Gynecology and Obstetrics (FIGO) recommendations on adolescent, preconception, and maternal nutrition:“Think Nutrition First”#. International Journal of Gynecology & Obstetrics. 2015;131:S213-S53. doi:https://doi.org/10.1016/S0020-7292(15)30034-5
- Wolff GL, Kodell RL, Moore SR, Cooney CA. Maternal epigenetics and methyl supplements affect agouti gene expression in Avy/a mice. The FASEB Journal. 1998;12(11):949-57. doi:https://doi.org/10.1096/fasebj.12.11.949
- Smith AD, Kim Y-I, Refsum H. Is folic acid good for everyone? The American journal of clinical nutrition. 2008;87(3):517-33. doi:https://doi.org/10.1093/ajcn/87.3.517
- Ferrazzi E, Tiso G, Di Martino D. Folic acid versus 5- methyl tetrahydrofolate supplementation in pregnancy. European journal of obstetrics, gynecology, and reproductive biology. 2020;253:312-9. doi:https://doi.org/10.1016/j.ejogrb.2020.06.012
- Bjelakovic G, Stojanovic I, Jevtovic-Stoimenov T, Bjelakovic L, Kamenov B, Pavlovic D, et al. Is folic acid supplementation to food benefit or risk for human health? Pteridines. 2013;24:3-4. doi:https://doi.org/10.1515/pterid-2013-0024
- Smith AD, Kim YI, Refsum H. Is folic acid good for everyone? American Journal of Clinical Nutrition. 2008;87(3):517-33.
- Blom HJ, Smulders Y. Overview of homocysteine and folate metabolism. With special references to cardiovascular disease and neural tube defects. Journal of Inherited Metabolic Disease. 2011;34(1):75-81. doi:https://doi.org/10.1007/s10545-010-9177-4
- Cochrane KM, Mayer C, Devlin AM, Elango R, Hutcheon JA, Karakochuk CD. Is natural (6 S)-5-methyltetrahydrofolic acid as effective as synthetic folic acid in increasing serum and red blood cell folate concentrations during pregnancy? A proof-of-concept pilot study. Trials. 2020;21:1-12. doi:https://doi.org/10.1186/s13063-020-04320-3
- Bailey SW, Ayling JE. The extremely slow and variable activity of dihydrofolate reductase in human liver and its implications for high folic acid intake. Proceedings of the National Academy of Sciences. 2009;106(36):15424-9.
- Scaglione F, Panzavolta G. Folate, folic acid and 5-methyltetrahydrofolate are not the same thing. Xenobiotica. 2014;44(5):480-8. doi:https://doi.org/10.3109/00498254.2013.845705
- Obeid R, Herrmann W. The emerging role of unmetabolized folic acid in human diseases: myth or reality? Current drug metabolism. 2012;13(8):1184-95.
- Kelly P, McPartlin J, Goggins M, Weir DG, Scott JM. Unmetabolized folic acid in serum: acute studies in subjects consuming fortified food and supplements. The American journal of clinical nutrition. 1997;65(6):1790-5. doi:https://doi.org/10.1093/ajcn/65.6.1790
- Maruvada P, Stover PJ, Mason JB, Bailey RL, Davis CD, Field MS, et al. Knowledge gaps in understanding the metabolic and clinical effects of excess folates/folic acid: a summary, and perspectives, from an NIH workshop. The American journal of clinical nutrition. 2020. doi:https://doi.org/10.1093/ajcn/nqaa259
- Morris MS, Jacques PF, Rosenberg IH, Selhub J. Circulating unmetabolized folic acid and 5-methyltetrahydrofolate in relation to anemia, macrocytosis, and cognitive test performance in American seniors. The American journal of clinical nutrition. 2010;91(6):1733-44. doi:https://doi.org/10.3945/ajcn.2009.28671
- Sweeney MR, Staines A, Daly L, Traynor A, Daly S, Bailey SW, et al. Persistent circulating unmetabolised folic acid in a setting of liberal voluntary folic acid fortification. Implications for further mandatory fortification? BMC Public Health. 2009;9(1):295.
- Sweeney MR, McPartlin J, Weir DG, Daly L, Scott JM. Postprandial serum folic acid response to multiple doses of folic acid in fortified bread. Br J Nutr. 2006;95(1):145-51. doi:https://doi.org/10.1079/bjn20051618
- Sweeney MR, McPartlin J, Weir DG, Scott JM. Measurements of sub-nanomolar concentrations of unmetabolised folic acid in serum. J Chromatogr B Analyt Technol Biomed Life Sci. 2003;788(1):187-91. doi:10.1016/s1570-0232(02)01010-3
- Bell KN, Oakley GP, Jr. Update on prevention of folic acid-preventable spina bifida and anencephaly. Birth Defects Res A Clin Mol Teratol. 2009;85(1):102-7. doi:https://doi.org/10.1002/bdra.20504
- Department of Health. Folate. 2010.
- Kim YI. Will mandatory folic acid fortification prevent or promote cancer? The American journal of clinical nutrition. 2004;80(5):1123-8. doi:https://doi.org/10.1093/ajcn/80.5.1123
- Lamers Y, Prinz-Langenohl R, Bramswig S, Pietrzik K. Red blood cell folate concentrations increase more after supplementation with [6S]-5-methyltetrahydrofolate than with folic acid in women of childbearing age. The American journal of clinical nutrition. 2006;84(1):156-61. doi:https://doi.org/10.1093/ajcn/84.1.156
- Tafuri L, Servy E, Menezo Y. The hazards of excessive folic acid intake in MTHFR gene mutation carriers: An obstetric and gynecological perspective. Clinical Obstetrics, Gynecology and Reproductive Medicine. 2018;4. doi:https://doi.org/10.15761/COGRM.1000215